🚨 What is happening in Fairfax County?! 🚨 Nothing…just ADULT MALE illegal immigrants going to high school with your daughters & molesting them!😳@EmeraldRobinson & I discuss the arrest of Israel Flores Ortiz, 19, for NINE COUNTS of sexual battery at Fairfax High on… — Stacy Langton (@MamaGrizzlyOrg) March 19, 2026
Unidentified drones spotted over DC Military base housing both the Secretary of State and Secretary of War.
Unidentified drones spotted over DC Military base housing both the Secretary of State and Secretary of War. — Douglas Macgregor (@DougAMacgregor) March 19, 2026
Free Speech for Me But Not for Thee
Last week, the chair of the Federal Communications Commission threatened to rescind the broadcast licenses of media entities that do not relate events in Iran or Ukraine as the Trump administration would like them to be related. He also attacked The Wall Street Journal and The New York Times for the same reasons. This followed […]
When Models Replace Reality in Modern Cosmology
The dominant scientific narratives about the universe may be revealing more about the assumptions built into their models than about the universe itself. The Expanding Gap Between Observation and Theory Modern cosmology is often presented as one of the great triumphs of contemporary science. Yet the deeper one looks, the more its explanations appear to […]
Butyrate and GLP-1 — Dual Messengers Linking Gut Health to Brain Health
Butyrate is a short-chain fatty acid (SCFA) produced in your gut when beneficial bacteria ferment dietary fiber that your body cannot digest on its own. As the primary energy source for colonocytes (the cells lining your colon), butyrate provides up to 70% of their energy needs.1
Butyrate directly nourishes the L-cells in your intestinal lining — the same cells that release GLP-1 after meals. GLP-1 is a hormone known for its role as a master regulator of metabolic health. It enhances insulin release after meals, suppresses glucagon, slows gastric emptying, and promotes satiety2,3,4,5 — all of which support blood sugar control and appetite regulation.
The butyrate–GLP-1 axis plays a key role in this natural system by fueling the L-cells that produce GLP-1. In addition to supporting GLP-1 signaling, butyrate also enhances energy expenditure by boosting fat oxidation and thermogenesis in brown adipose tissue.6,7 Animal studies reinforce these benefits: in mice fed a high-fat diet, butyrate supplementation significantly improved glucose metabolism and prevented weight gain.8
Pharmaceutical GLP-1 agonists attempt to mimic this effect, but your body already possesses a mechanism to produce GLP-1 on its own — provided L-cells receive sufficient fuel. Butyrate activates free fatty acid receptors on L-cells, which directly stimulate GLP-1 secretion.
Research shows that reduced butyrate availability leads to lower GLP-1 output, impaired insulin sensitivity, increased appetite, and greater fat accumulation.9 In this framework, obesity reflects a breakdown in microbial fuel delivery rather than a failure of calorie control alone. The steps needed to rebuild and support this natural mechanism is the central topic of my new book, “Weight Loss Cure; Melt Fat Naturally With Your Own GLP-1.”
How Butyrate Supports Your Body’s Built-In GLP-1 System for Weight and Mood
When butyrate is abundant, GLP-1 secretion follows the body’s original blueprint without external intervention:
• It slows gastric emptying, so you feel full longer
• It reduces glucagon, which lowers blood sugar
• It enhances insulin sensitivity and helps your body burn fat
• It sends satiety signals to the brain, curbing cravings and emotional eating
• It activates GLP-1 receptors in the brain, where it helps regulate mood, reduce anxiety, and support cognitive health
Butyrate and GLP-1 Are the Natural Design
Importantly, you don’t need a synthetic GLP-1 agonist to access these benefits. You need butyrate. This is how human metabolism was designed to work — not with synthetic shots, but with internal balance.
Your L-cells are engineered to release GLP-1 in response to butyrate. When the gut microbiome is balanced and well-fed with fermentable fiber, GLP-1 production activates after meals to regulate appetite, support insulin release, and promote fat burning — all without a prescription.
This design evolved to work in harmony with ancestral diets rich in whole foods, fiber, and unprocessed carbohydrates. Disruption to this design breaks the microbial fuel line, not the hormonal hardware.
When you restore butyrate production, you remove the blockages and reactivate the normal regulatory feedback loop, which lets your built-in weight regulation system function again, as intended. Whether you’re exploring medication options or want to support your body’s own systems, restoring butyrate production is foundational to how this hormone was designed to work.
How This System Gets Disrupted
Modern lifestyles disrupt this elegant mechanism. Seed oils, which are high in the omega-6 fat linoleic acid (LA), damage your gut lining and deplete butyrate-producing microbes. Low-fiber, high-sugar diets feed the wrong bacteria. Chronic stress and poor sleep reduce microbial diversity. All of this breaks the link between fiber, butyrate, and GLP-1. The result? Your natural weight regulation system goes offline.
Butyrate and GLP-1 Also Support Brain Health
Butyrate also helps regulate how your gut communicates with your brain, supporting the normal stress, immune, and mood responses your body was designed to manage.
As a key signaling molecule in the gut-brain axis, butyrate helps regulate the stress response, increase pain tolerance, and reduce neuroinflammation. It even crosses the blood-brain barrier, where it supports brain-derived neurotrophic factor (BDNF), boosts mitochondrial function, and protects against depression and cognitive decline.
GLP-1 is also more than a metabolic hormone. Like butyrate, it’s a brain-active compound.10 GLP-1 receptors are found in areas of the brain that govern memory, mood, and motivation. Activating them can reduce anxiety, blunt inflammation, and improve neuroplasticity.11,12
Together, butyrate and GLP-1 act as dual messengers — one produced by your gut microbes, the other released in response to it. They work in tandem to support the natural coordination of metabolism, immune function, and mental health, restoring the biological systems your body relies on to stay balanced.
How Butyrate’s and GLP-1 Inhibit Neuroinflammation
Neuroinflammation is widely recognized as a key factor in the development and progression of a wide range of neurodegenerative diseases, including Alzheimer’s disease, Parkinson’s disease, and multiple sclerosis (MS).
A meta-analysis published in Neuroscience Letters,13 reports that butyrate supports brain health through multiple gut-brain mechanisms, particularly by strengthening mitochondrial function in the brain after fiber fermentation.
Butyrate suppresses major inflammatory pathways, most notably nuclear factor kappa-light-chain-enhancer of activated B cells (NF-κB),14 a master regulator of inflammation. In experimental models of Parkinson’s disease, beta-hydroxybutyrate reduced inflammation, protected neurons from endotoxin injury, and improved behavioral outcomes. By limiting NF-κB activity, butyrate lowers inflammatory cytokine release, which helps preserve synaptic function.
Butyrate also inhibits histone deacetylases (HDACs),15 which alters gene expression in brain cells. This epigenetic effect reduces pro-inflammatory signaling while increasing anti-inflammatory pathways, further calming neuroinflammation.16 In animal models of Alzheimer’s disease, butyrate lowered amyloid-beta plaque accumulation by up to 40% and supported cognitive performance.17
Butyrate-driven GLP-1 release adds another layer of protection. Preclinical research shows GLP-1 shields dopamine-producing neurons in Parkinson’s disease by lowering oxidative stress and supporting mitochondrial energy production.18 GLP-1 also promotes autophagy,19,20 which clears damaged proteins such as alpha-synuclein, and enhances insulin sensitivity and cellular energy metabolism in the brain,21 which is often impaired in Parkinson’s disease.
Butyrate, Mood, and the Gut-Brain Connection
Butyrate also influences mood and cognition by acting on key neurotransmitters, brain growth factors, and the vagus nerve. It enhances the production of gamma-aminobutyric acid (GABA) and dopamine22 — two crucial messengers that calm the nervous system and promote motivation and emotional balance. Low butyrate levels have been linked to anxiety and depression,23 in part due to disrupted gut-brain signaling.
As mentioned, it also boosts BDNF, a growth factor vital for learning, memory, and neuroplasticity.24,25 By inhibiting HDACs, butyrate increases BDNF in brain regions like the hippocampus, supporting neuron growth and reducing inflammation-driven damage.26 Low BDNF is a common feature in conditions like Alzheimer’s and major depression.27,28
Butyrate further strengthens the gut-brain axis by activating the vagus nerve — a communication superhighway that calms the body, lowers inflammation, and regulates neurotransmitters like serotonin and GABA.29 Increased vagal tone is associated with improved mood, better stress tolerance, and enhanced digestion, making butyrate a central player in emotional and cognitive health.30
How to Restore Butyrate Production in Your Gut
To restore your body’s natural weight management and mood regulation systems, you need to restore and support the bacteria in your gut that produce butyrate and other SCFAs. Here’s how:
1. Start with gut terrain repair — If you’re bloated, constipated, or sensitive to high-fiber foods, you need to calm inflammation before you feed the microbiome. That means:
• Avoiding fermentable fibers at first. When your gut is out of balance, high-fiber foods — even the “healthy” ones — can work against you. Foods like beans, lentils, oats and raw greens ferment quickly when the wrong bacteria are in control. This creates gas, pressure and inflammation, and worsens gut lining damage.
• Eliminating seed oils (such as soybean, corn, canola, sunflower). LA damages the exact gut microbes you’re trying to support. If your diet includes fried foods, processed snacks or sauces made with soybean, corn, sunflower, or canola oil, you’re suffocating your good gut bacteria. Replace those fats with ghee, grass fed butter, or tallow — fats your body actually knows how to use. The goal is to shift your internal terrain so your gut bacteria thrive again.
• Using simple carbs like white rice and ripe fruit to stabilize energy without feeding bad bacteria.
2. Reintroduce fiber in phases — Move on to fiber reintroduction only after you meet this criterion: You tolerate three consecutive days of white rice or ripe fruit with no bloating, abdominal pain, excess gas, or bowel urgency. At that point, introduce one resistant starch source at a time, starting with 1/2 cup cooked-and-cooled white potato once daily.
Once you can consume 1/2 cup cooked-and-cooled potato daily for seven consecutive days with no increase in gas, bloating, stool looseness, or abdominal discomfort, advance to inulin-rich foods such as garlic, onions and leeks. These fibers bypass digestion in your small intestine and head straight to your colon, where they fuel beneficial bacteria that make butyrate.
3. Support with optional tools — Once your gut begins to stabilize, these targeted tools can help accelerate butyrate production and improve results:
• Phase 1 — Akkermansia postbiotics — Postbiotics are non-living bacterial components that still deliver biological signals. Pasteurized forms of Akkermansia muciniphila contain Amuc_1100, a protein shown to tighten the gut barrier and reduce inflammation. Look for postbiotic formulas with enteric coating or microencapsulation to ensure they survive stomach acid and reach the colon intact.
Without that protection, less than 5% of Amuc_1100 reaches your colon. You could try megadosing to compensate, but that’s expensive and inefficient. Prioritize coated formats to support your gut barrier more effectively.
• Phase 2 — Live Akkermansia — Begin Phase 2 probiotics only after all of the following occur:
◦Bloating remains minimal or absent
◦Stool form stays consistent for at least 7 days
◦Fiber tolerance expands without symptom return
In this stage, introduce live probiotic Akkermansia alongside gentle prebiotics — like small amounts of resistant starch — to support the growth of butyrate-producing strains and reestablish a healthy, oxygen-sensitive microbial environment.
• Fermented foods — Raw sauerkraut, kefir, and other traditionally fermented foods can boost microbial diversity and support butyrate-producing strains. Go slowly — start with small amounts to test tolerance, especially if your gut is sensitive.
• Gut testing — A stool analysis can reveal which bacteria are present, whether your gut is inflamed, and how well you’re producing short-chain fatty acids like butyrate. This can guide food choices and supplementation more precisely.
• Resistant starch — Found naturally in cooked-and-cooled potatoes, green bananas, and legumes — or as supplemental powders — resistant starch bypasses digestion in the small intestine and becomes prime fuel for butyrate-producing bacteria in the colon.
4. Adjust your environment — Your gut doesn’t just respond to what you eat. It’s tuned into your entire lifestyle. These daily habits help create the internal rhythm your microbiome needs to thrive:
• Sleep — Align your sleep-wake cycle with natural light exposure. Aim for 7 to 9 hours of high-quality sleep and get morning sun to anchor your circadian rhythm. This helps regulate gut motility and microbial repair.
• Stress — Chronic stress alters your microbiome and shuts down butyrate production. Use daily tools like breathwork, walking outdoors, and nervous system regulation practices to calm your hypothalamic-pituitary-adrenal (HPA) axis and support microbial balance.
• Fasting window — Stop eating at least three hours before bed. This gives your migrating motor complex (MMC) — your gut’s internal clean-up crew — time to sweep out bacteria and food debris overnight, reducing fermentation and inflammation.
Signs Your Gut Is Making More Butyrate
The following improvements reflect rising butyrate levels and gut healing in real time:
• Bowel movements become regular and well-formed — A sign of improved colonic motility and mucosal integrity.
• Fiber tolerance improves — Less bloating, gas, or discomfort after meals rich in fermentable fiber.
• Hunger fades between meals — As GLP-1 and PYY production increases, satiety naturally extends.
• Mood feels more stable and stress less overwhelming — Butyrate supports BDNF and modulates the HPA axis.
• You lose fat without trying to eat less — Improved metabolic signaling leads to spontaneous caloric reduction.
• Reduced post-meal blood sugar spikes — A measurable effect tied to improved insulin sensitivity and GLP-1 response.
• Lower fasting insulin and triglycerides (if tested) — Both improve with SCFA restoration and microbiome balance.
• Fewer cravings for processed carbs and snacks — Satiety hormones rise while inflammation-driven hunger decreases.
• Less urgency or discomfort with bowel movements — Improved stool consistency reflects stronger gut barrier and reduced inflammation.
• Improved breath or reduction in sulfur/gas odors — Indicates better fermentation profile in the colon (fewer sulfur-releasing or proteolytic bacteria).
Track Your Progress: How to Know It’s Working
To track your recovery, keep a simple symptom journal for the first four to six weeks. Each day, jot down quick notes on these four markers:
• Bloating — None, mild, moderate, or severe
• Energy — Steady, sluggish, or crashing
• Mood — Calm, tense, irritable, anxious
• Bowel quality — Bristol stool scale (types 3 to 4 are ideal), frequency, urgency, discomfort
Even just a few words per day can help you see patterns clearly, especially when deciding when to add new foods or supplements. Once you begin reintroducing fermentable fiber, use a 1 to 10 scale each week to rate how well you’re tolerating it. If you’re not at a 7 or above, pause before advancing to the next phase.
• 1 = severe gas, bloating, or pain
• 5 = some symptoms, improving
• 10 = no symptoms, excellent digestion
If you want objective data, run these labs at baseline and again around week 8. These markers, while optional, offer biochemical confirmation that your butyrate–GLP-1 axis is restoring normal metabolic function.
• Fasting insulin — Falling levels suggest better GLP-1 signaling
• Triglycerides — Often improve as inflammation and insulin resistance drop
• Post-meal glucose — Ideally stays under 120 mg/dL at the 1-hour mark
Timeline: What to Expect as Your Gut Rebuilds
Your gut already knows how to help you lose weight — by producing butyrate, which fuels the cells that make GLP-1. This is how human metabolism was designed to function. Restore that system, and your cravings shrink, your blood sugar stabilizes, your inflammation calms down, and your body starts releasing excess weight naturally.
These shifts are clear signs that your body’s metabolic software is running the way it was meant to. Your gut doesn’t need to be perfect to start producing butyrate. But there’s a rhythm to recovery, and markers to know it’s working.
Phase
What Happens
Timeframe
Measurable Indicators
Terrain repair
Gas, bloating, and sensitivity begin to calm
1 to 3 weeks
Less urgency, firmer stools, more predictable digestion
Fiber reintroduction
Butyrate-producing strains begin to increase
2 to 4 weeks
Better tolerance of resistant starch, mood uplift
GLP-1 response
Appetite regulates, energy improves, cravings decrease
4 to 8 weeks
Fewer between-meal snacks, better AM energy
Metabolic reset
Satiety increases, fat loss begins, blood sugar stabilizes
6 to 12 weeks
Tighter waistline, reduced post-meal glucose swings
You can start putting these strategies into practice right now with my new book, “Weight Loss Cure; Melt Fat Naturally With Your Own GLP-1,” which provides a step-by-step plan to rebuild butyrate production, restore natural GLP-1 signaling, and correct the root drivers of weight gain. We’re also preparing a butyrate-support product designed to complement these foundational strategies. You can join the waitlist now, and when it becomes available, you’ll receive a $5 off coupon by email.
The Wide, Encompassing Role of Vitamin K2 on Human Health
A New Series of Health Insights Is on the Way
WAŻNY
A New Series of Health Insights Is on the Way
Our team has been working behind the scenes to prepare new research and practical health
strategies for our readers. While we finish preparing what’s coming next, we invite you to
explore one of the most-read articles from our library below. See exactly what’s changing →
When it comes to vitamins, well-known examples that immediately come to mind include vitamins C and D. While these are certainly important, I believe that other vitamins also deserve their own spotlight, such as vitamin K2.
In this episode of the Wellness by Designs podcast, nutritionist Brad McEwen, Ph.D., explains the role of vitamin K2 in your body, and what happens when you don’t get enough of this nutrient.
How Vascular Calcification Occurs When You’re Deficient in Vitamin K2
One of the most significant benefits of vitamin K2 is its ability to support cardiovascular health. When calcium builds up in your arteries, it leads to stiffening and blockages.
• The importance of vitamin K2 for optimal cardiovascular health — Research shows that it activates biological processes that direct calcium away from your arteries and into your bones and other essential organs, but a deficiency can increase your risk of cardiovascular disease.
McEwen explains further,1 “One of the areas we’ve been looking at is a deficiency of vitamin K2 has been linked to vascular calcification. Not just coronary, but just overall calcification. And if you think of it this way, you got different mineral deposition, particularly calcium, of course, coming from the calcium hydroxyapatite — and we always say from the bones because that’s the main storage site into the vascular system and then going into the vascular wall because it gets trapped.”
• Blockage occurs due to the molecular weight of calcium — McEwen theorizes that the heaviness of calcium contributes to its propensity to cause arterial blockages.
“So, it’s like a big centrifugal force going through the arteries and then it just gets trapped because it’s, I don’t know, heavier? It’s like a big metal going through and then it embeds and over time, as you know, we talk about foam cells, atherosclerosis, etc., and it starts that calcium, you know, process,” he says.
From there, McEwen describes where the calcium actually embeds in your cardiovascular system, increasing your risk for clots that eventually block blood flow:2
“The biochemistry all combines together leading to this complex which, then, sat in the arteries and it can sit in the basement membrane of the artery. It can be on the inner or outer side of that membrane, leading to an inflammatory process and oxidative process, leading to like a firestorm in there.
The body tries to heal it, you know, by laying down fibrin and different connective tissue to protect it — putting a Band-Aid down, I suppose. And then that’s when you get your atherosclerosis, your plaque formation and then your eventual clot in that area.”
Heavy Metals Increase the Risk of Vascular Calcification Further
It’s not just a lack of vitamin K2 that increases your risk for vascular calcification. Even the very environment you live in influences your risk. McEwen recounts a case study related to this observation, wherein he saw a patient whose previous physicians couldn’t figure out what was happening with her despite trying out “every test under the sun.”3
• Heavy metals embed into your tissues — McEwen discovered that it was due to the presence of heavy metals in her childhood neighborhood, which embedded into her tissues. When she moved out of the area, the heavy metals circulated throughout her system, causing bone pain and increasing cardiovascular risk.
• Nutritional deficiencies contribute to vascular calcification via heavy metal exposure — According to McEwen, bone-related nutrient deficiencies do not direct calcium to where it’s needed the most.
“What I found out was due to her childhood, there was different heavy metals in the area, and that’s what deposited into the tissue. And when she moved around, that tissue left — because she didn’t have enough vitamin D, vitamin K, etc. — and then left the bone, so she had bone pain, and then embedded into her vascular system leading to cardiovascular link,” he says.4
Research Surrounding the Benefits of Vitamin K2
The benefits of vitamin K2 regarding cardiovascular health have been well-studied for many years now.
• Vitamin K2 makes your arteries more elastic — McEwen cited a study that involved 244 healthy postmenopausal women. Split into two groups, the test group (120 participants) took 180 micrograms of vitamin K2, and the control group (124 participants) took a placebo for a total of three years. After the study was completed, McEwen noted that the test group had improved arterial flexibility.5
• Increased vitamin K2 consumption helps improve other metabolic health markers — In another study, researchers followed 36,629 participants for 12 years and monitored their vitamin K2 intake. They found that those with a higher intake of vitamin K2 had a 29% lower risk of developing peripheral artery disease. Other improvements were noticed as well, including a 44% reduction in Type 2 diabetes risk, and a 41% reduction in high blood pressure.6
• The benefits of vitamin K2 on mitochondrial function — A study published in Open Heart journal showed that people with higher levels of K2 in their diet tend to have lower levels of arterial calcification and a reduced risk of heart disease.
Higher K2 levels also had a positive impact on mitochondrial health, particularly for cardiac muscles. “The role of vitamin K2 in mitochondrial function is mediated by its production of mitochondrial ATP, which has direct implications for contractile muscles (i.e., cardiac) that are comprised of abundant mitochondria.
Intake of vitamin K2 has been associated with increased cardiac output, stroke volume and heart rate and decreased blood lactate. These effects are consistent with the greater maximal cardiovascular performance seen with oral vitamin K2 supplementation, according to the researchers.”7
How Vitamin K2 Helps Strengthen Your Bones
Vitamin K2 is also essential for maintaining strong and healthy bones. Your bones are constantly breaking down and rebuilding, a process that relies on proper calcium distribution.
• Vitamin K2 activates bone-forming proteins — Research shows vitamin K2 helps promote osteocalcin, which is a protein that binds calcium to your bone matrix. Without enough vitamin K2, your bones will not be as strong as they should be, increasing your risk of fractures and osteoporosis.8
• Osteocalcin serves as the calcium guide — McEwen notes that osteocalcin, a vitamin K-dependent protein, helps promote stronger bones by transporting calcium to where it actually needs to go — your skeleton. Your body needs a constant influx of this all the time because it is always building itself up and removing old, damaged bone cells.9
The Sweet Spot Dosage of Vitamin K2
If you’re considering adding vitamin K2 to your diet, it’s important to get the right amount.
• Vitamin K2 requirements vary for different age groups — According to McEwen, much of the research he has studied had dosages between 90 and 180 micrograms per day, which he believes is the optimal for most adults.10 Youngsters and teenagers (10 to 18 years old) need around 90 micrograms, while children below the age of 10 need 45 micrograms.11
While some studies have explored higher doses, the standard recommendation is based on what has been shown to be effective without unnecessary excess.
• Find the ideal range based on your health needs — While McEwen recommends different ranges, he clarifies further by saying that the dosage will vary from person to person.
McEwen also mentioned another important precaution — taking excessively high doses of vitamin K2 won’t be good for your health because your body won’t be able to use it all:12
“One thing I always want to say when we do podcasts, and everything is it’s always the person in front of you. ‘What is the best dose for that person?’ And if they need 500 IUs of vitamin D and 90 micrograms of vitamin K2 from your determination, that’s the dosage that they need.
If they need a higher dose of, you know, 1,000 IUs of vitamin D3 and 180 micrograms of K2, that’s the dose regimen … [G]oing hard and fast is not always the best way to do it because, to me, it’s trying to push too much through all the time.
We get excited, some studies are very, very high dose and they seem to have the negative impact because, I believe, the regulatory pathways are not able to function effectively to make sure we get the best out of what it is.”
From McEwen’s statement above, you’re thinking, “What does vitamin D have to do with this entire process?” Well, vitamin D has been shown to play a role in calcium absorption. If you’re deficient in this important nutrient, your risk for rickets, a disease marked by skeletal deformities, increases.13 With enough vitamin D and vitamin K2, the calcium you get from your diet will go to the right organs.
Strategies to Ensure Your Body Gets Enough Vitamin K2
Based on McEwen’s findings, it’s clear that vitamin K2 has an important role in your body as it influences a wide range of functions, such as cardiovascular and skeletal health. The good news is that boosting your vitamin K2 levels is inexpensive and practical to implement. Here are my recommendations:
1. Add more K2-rich foods into your diet — The best way to get more vitamin K2 is through your diet, and they’re found in many foods. Nutritious choices include fermented foods like natto, aged cheeses (especially gouda and brie), egg yolks, and grass fed dairy products. Beef ideally organic and grass fed, also contains vitamin K2.14
2. Support your gut health for better vitamin K2 production — Your gut bacteria actually produce some of the vitamin K2 your body uses, but they need the right environment to thrive. If your digestion isn’t working well, or if you’ve been on antibiotics recently, you might not be making enough K2 on your own.
To support your gut, eat more fermented foods like sauerkraut, kimchi, and kefir, which provide the right bacteria to help your gut naturally produce K2. Also, make sure you’re eating plenty of fiber from vegetables and whole fruits to nourish the gut bacteria already active in your gut.
3. Pair K2 with vitamin D — As noted by McEwen, vitamin K2 and vitamin D work together to control the flow of calcium in your body — vitamin D helps boost absorption, while K2 makes sure it goes to the right places.
If you’re taking a vitamin D supplement but not getting enough K2, you’re increasing your calcium levels without giving your body the ability to direct it properly. If you’re already supplementing with D3, make sure you’re also getting enough K2, either through food or supplements to maintain proper homeostasis.
4. Stay active to keep your bones strong — Movement is key for keeping your bones in good shape. Weight-bearing exercises like walking, strength training, and bodyweight exercises help signal your body to send calcium into your bones where it belongs.
As noted by McEwen, sitting for long periods without movement also changes your bone mineral density, and all the vitamins K2 and D you’ve been taking will be for nothing.15 If you spend a lot of time sitting, I encourage you to go for a walk outside to boost your fitness levels.
5. Take a high-quality vitamin K2 supplement if needed — If you’re not getting enough K2 from your food, adding a supplement is a viable way to ensure you’re covered. Look for a supplement that contains MK7, as this form stays in your body longer and is more effective than other types. For best results, take it with a meal that contains healthy fat, as K2 is a fat-soluble vitamin.
FAQ — Common Questions About Vitamin K2
Q: What is vitamin K2 and why is it important?
A: Vitamin K2 plays a crucial role in calcium metabolism. It helps prevent vascular calcification by directing calcium away from arteries and into bones, reducing the risk of heart disease and arterial stiffness. Additionally, it supports bone health by strengthening bone density and reducing the risk of fractures and osteoporosis.
Q: How does vitamin K2 benefit cardiovascular health?
A: Vitamin K2 activates proteins that prevent calcium buildup in the arteries, reducing the risk of vascular calcification, atherosclerosis, and blood clots. Research shows that people with higher vitamin K2 intake have a 29% lower risk of peripheral artery disease, a 44% reduction in Type 2 diabetes risk, and a 41% reduction in hypertension.16
Q: What are the best dietary sources of vitamin K2?
A: Good sources of vitamin K2 include fermented foods (like natto and aged cheeses), pastured egg yolks, grass fed dairy products, and organic, grass fed beef. Your very own gut bacteria also produce some vitamin K2, which is further supported by consuming probiotics and fiber-rich foods.
Q: What is the recommended daily intake of vitamin K2?
A: The general range for adults is 90 to 180 micrograms per day, while the range for children 10 to 18 years old is 90 micrograms per day. For children up to 10 years old, the dosage is 45 micrograms per day.
Q: How can I ensure optimal vitamin K2 levels?
A: To maintain adequate vitamin K2 levels, support your gut health with fermented foods and fiber and pair it with vitamin D for better calcium absorption. Take a high-quality supplement if dietary intake is insufficient.
1 in 10 Deaths from Infectious Disease Are Caused by Obesity
Obesity continues to be a problem in America. According to the U.S. Centers for Disease Control and Prevention (CDC), 73.6% of adults 20 years and older are overweight and obese.1 This staggering number is putting serious strain on the economy, leading to a whopping $1.4 trillion in annual health expenses.2 Having excess body fat causes an assortment of health complications to arise, including high blood pressure, heart disease, stroke, metabolic syndrome, fatty liver disease, and Type 2 diabetes.3
While these complications have been extensively studied within the context of obesity, they are metabolic in nature. Another part that’s rarely discussed is the impact of obesity on infectious disease — complications caused by microbes. Now, a study published in The Lancet attempts to answer this mystery.
Obesity Drives a Measurable Rise in Severe Infection Risk
The researchers explored how obesity affects your risk of mortality. The rationale for following this line of research was because the metabolic effects of obesity have already been extensively covered, but much less is known about its impact across different types of infectious diseases.4
For the analysis, the researchers selected 67,766 adults from two Finnish cohort studies and 479,498 adults from the United Kingdom (U.K.) Biobank. The participants’ body mass index (BMI) was tracked at baseline — 1998 to 2002 for the Finnish population and 2006 to 2010 for the U.K. population. Infection-related mortality risk due to obesity was analyzed until 2018, 2021, and 2023 — before, during, and after the COVID-19 pandemic.
• Mortality risk steadily climbed as BMI increased — People in the highest obesity class had a 2.75 times higher risk for severe nonfatal infections in the Finnish cohorts and 3.07 in the U.K. Biobank, meaning triple the risk compared to adults at a healthy weight.
For fatal infections, the danger was even higher. The risk reached 3.06 times in Finland and 3.54 times in the U.K., underscoring the magnitude of this problem.
• About 1 in 10 deaths from infectious disease are caused by obesity — After modeling the global impact, the researchers reported that 8.6% of all infection-related deaths in 2018 were attributable to obesity, rising to 15.0% during 2021 and settling at 10.8% (0.6 million out of 5.4 million) in 2023 as global conditions shifted due to the COVID-19 pandemic.
Another striking detail lies in how consistent the findings were across measurement methods. When the researchers evaluated obesity using waist circumference, waist-to-hip ratio, and body fat percentage, the risk remained almost identical — 1.7 times for severe infection across metrics. In short, excess fat, no matter how it’s measured, puts your health at risk.
• Infection severity was closely linked to obesity — The analyses included long follow-up periods, and captured infection events before, during, and after the COVID pandemic. Across all eras, the pattern held. Even when the COVID-19 pandemic entered the picture, the underlying risk landscape hardly budged.
Some groups experienced even steeper risk elevations than others. While the study reports strong effects across nearly everyone with obesity, individuals with class III obesity faced the largest surge in both hospitalizations and deaths.
• For context, obesity is currently broken down into three classes — Class I is a BMI of 30 to 34.9, and class II is a BMI of 35.0 to 39.9. Lastly, class III refers to a BMI of 40 or higher.5 Moving from overweight (BMI between 25 and 29.9) to class I obesity created a measurable rise in risk. However, advancing to class II and class III amplified the danger sharply.
• Excess fat tissue upsets metabolic health by keeping your body in a constant low-grade inflammatory state — As a result, immune function is also affected. According to the researchers, these include “[r]educed T-cell and NK-cell function, neutrophil dysfunction, dysregulated complement and adiponectin signalling, and diminished mucus clearance and lymphatic flow.”
A Deeper Look at How Obesity Affects Your Risk for Infectious Disease
In the previous study, researchers analyzed the risk that obesity poses to your health when it comes to infectious disease. Now, it’s time to look at the biological mechanisms involved. In another study published in the International Journal of Obesity, researchers outlined different ways excess body fat reshapes your immune function and becomes vulnerable to infections.6
• Higher body fat percentage equals higher infectious disease risk — The study reported the same pattern seen in The Lancet study — infections did not just simply occur more often in individuals with obesity; they progressed more aggressively.
According to the authors, “obesity has substantial effects on the immune system,” meaning the body’s internal security system struggles to respond effectively once pathogens enter when excess body fat gets in the way. The image below provides a summary of their theories:
Source: International Journal of Obesity volume 46, pages 449 to 465 (2022)
• Excess adipose tissues (body fat) behave like an active endocrine organ — They release inflammatory hormones and chemical signals that disrupt communication between immune cells. In plain terms, the immune system loses coordination. When you live with this imbalance, you face a slower response to viruses and bacteria, which allows these microbes to multiply more easily.
• Obesity alters the architecture and function of the respiratory system — The authors explained that excess fat around the chest wall reduces lung expansion and lowers lung volumes, creating a mechanical disadvantage when the body tries to clear mucus or maintain airflow during an infection.
If you’ve ever felt out of breath walking up a short flight of stairs, this is the same limitation playing out at a microscopic level during a bout of respiratory illness. Bacteria and viruses take advantage of that reduced airflow, settling deeper into lung tissues.
• Inflammation persists for years in many obese individuals — Over time, this constant inflammatory pressure exhausts their immune cells. The review highlights that macrophages — the immune cells responsible for engulfing and clearing pathogens — switch into a less effective mode of activity under the influence of obesity-related inflammation. Instead of clearing invaders quickly, macrophages operate sluggishly, which prolongs infections and increases tissue damage.
• Respiratory infections often worsen the fastest, but skin issues aren’t far behind — Altered circulation reduces the body’s ability to deliver immune cells to the site of injury. However, changes in the skin also slow down wound-healing, allowing bacteria to enter your system faster.
• Excess skin due to obesity increases risk for topical infections — As body fat begins to increase, the skin compensates accordingly and causes more skin folds. The researchers noted that these are factors that increase the risk of fungal and bacterial skin infections.
• Obese individuals usually have existing nutrient deficiencies, which worsen the problem further — For example, vitamin D deficiency is far more common in adults with obesity. This nutrient plays an important role in immune function, especially in controlling inflammation in the respiratory tract.
• Adipose tissue in obesity recruits immune cells into fat stores, diverting them from circulation — This means that your body’s main protectors are pulled away from where infections unfold. As a result, when a pathogen enters through the lungs, skin, or gut, fewer active immune cells are available to meet the threat. Your body ends up fighting with a depleted army:7
“In obesity, visceral adipose tissue produces an excess of cytokines such as tumour necrosis factor α (TNFα) and interleukin (IL)-6 and 1β that could weaken the response of immune cells during an infectious stimulus,” the researchers explained.
“In addition, in a state of excess weight, a condition of hyperleptinemia is observed that can contribute to immune imbalance.”
How to Restore Your Healthy Metabolism and Stop Fat Storage
As noted in the findings, excess body fat won’t do your health any good, and the best time to start getting rid of it is today. If you’ve been having difficulty losing weight despite your best efforts — be it exercising or modifying your diet — the problem is in your cellular energy function.
When your cells are saturated with polyunsaturated fats (PUFs) like linoleic acid (LA), your body lowers its metabolic rate, shifting into storing fat instead of burning it. Thus, the foundational step isn’t running countless miles because you can’t outrun a bad diet. The answer lies in fixing how your body burns fuel through corrective action by way of eating properly.
1. Remove vegetable oils from your diet — Every time you eat ultraprocessed foods or food cooked in soybean, canola, corn, safflower, or sunflower oil, you push more LA into your tissues, slowing down your cellular energy production and nudging your body toward metabolic hibernation.
Once you reduce and eliminate these unhealthy oils from your diet, your cells stop fighting the inflammatory load and start burning fuel with far less strain. As this shift settles in, you feel more stable because your mitochondria burn energy cleanly.
I recommend keeping your LA intake under 3 grams a day. This amount aligns with the intake that our ancestors had before the rise of industrially made vegetable oils. To help you with accurate monitoring, sign up for the Mercola Health Coach app once it becomes available. It will contain a feature called a Seed Oil Sleuth, which will compile your daily LA intake to a tenth of a gram.
2. Choose stable fats to keep energy steady — Continuing the point above, when you trade out seed oils for healthier saturated fats like grass fed butter, coconut oil, ghee, and beef tallow, you give your metabolism a major advantage. These fats burn cleanly, support oxygen use, and help your cells stay switched on instead of drifting into storage mode. It’s the difference between running your engine on premium fuel versus watered-down gasoline.
3. Choose healthy carbs to maintain metabolic flexibility — Don’t be tempted to cut out carbs in an effort to lose weight because this forces your body into a low-oxygen, low-energy environment. When chosen carefully, carbs, especially healthy ones, protect your metabolism. That means choosing whole fruits, white rice, and root vegetables — foods that help promote proper cellular energy. Don’t choose refined and ultraprocessed carb sources.
4. Dial down stress — Feeling tense, overstimulated, or wired, especially at night, usually means that your cortisol and estrogen are running too high, pushing your system toward fat storage and suppress healthy energy production.
To lower your stress levels, remember to get daily sunlight and restful sleep, and minimize back on alcohol (or remove it entirely). As those stress signals drop, your metabolism burns energy better instead of hoarding it.
5. Teach your body to switch metabolic fuels through exercise — Staying inactive teaches your mitochondria to conserve rather than produce. Doing gentle strength training, daily walking, and light resistance exercise can wake them back up.
Movement tells your cells how to use both fat and carbs for energy, instead of locking into one inefficient mode. You don’t need extreme exercise — you only need consistent motion that challenges your muscles and keeps energy flowing.
Frequently Asked Questions About Obesity-Related Infectious Disease Mortality
Q: How does obesity increase the risk of infectious disease?
A: Obesity creates chronic inflammation that impairs T-cells, NK-cells, and macrophages. Excess fat diverts immune cells into fat stores, while insulin resistance raises blood sugar, helping microbes spread.
Q: How much does obesity raise the risk of severe or fatal infections?
A: Research shows that people in the highest obesity class face up to 3.54 times the risk of fatal infections. Globally, about 1 in 10 infectious disease deaths are attributable to obesity.
Q: Why are respiratory infections especially dangerous for people with obesity?
A: Excess chest fat restricts lung expansion and airflow, making it harder to clear mucus. This allows bacteria and viruses to settle deeper into lung tissue and progress more aggressively.
Q: Does the type of obesity measurement matter when assessing infection risk?
A: No. Whether using BMI, waist circumference, waist-to-hip ratio, or body fat percentage, infection risk remained nearly identical — about 1.7 times higher across all metrics.
Q: What steps can reduce infection risk related to obesity?
A: Eliminating vegetable oils high in linoleic acid (LA), choosing stable fats and healthy carbohydrates, managing stress, and incorporating consistent gentle exercise to restore metabolic function all work together to help reduce excess body fat and protect your health.
Jeremiah in Ireland: Proof from the Bible and the Irish Annals
Jeremiah in Ireland Proof from the Bible and the Irish Annals by John E. Wall One of the most beloved stories of traditional literature written by those who support the modern identity of the Lost Ten Tribes of Israel is the story of the coming of the prophet Jeremiah to Ireland. According to this story […]
RT by @DougAMacgregor: The current defense policy, anchored in obsolete structures and strategies, is akin to a ship too costly to maintain and too rickety to sail the complex waters of the 21st-century. FULL ARTICLE: ➡️ pic.
The current defense policy, anchored in obsolete structures and strategies, is akin to a ship too costly to maintain and too rickety to sail the complex waters of the 21st-century. FULL ARTICLE: ➡️ https://t.co/THfUGXD0Df pic.twitter.com/mneRzQ7m7U — Douglas Macgregor (@DougAMacgregor) March 18, 2026
BREAKING: MacDill Air Force Base in Tampa, home to U.S. Central Command (CENTCOM) under shelter-in-place order over threat.
BREAKING: MacDill Air Force Base in Tampa, home to U.S. Central Command (CENTCOM) under shelter-in-place order over threat. — Douglas Macgregor (@DougAMacgregor) March 18, 2026
IMEC: Trump’s War With Iran Is About Global Trade. Period.
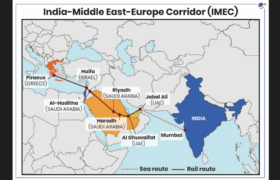
I wrote this white paper to lay bare the myths surrounding the war in Iran and to expose the master plan to restructure global trade routes in order to dominate world trade. This is a tectonic shift in the geopolitical structure of the world. Further, this is the master plan for global Technocracy, even down to making Gaza into the poster child for the technocratic
Cluster Bomb slams Tel-Aviv, at least 2 reported dead.
Cluster Bomb slams Tel-Aviv, at least 2 reported dead. — Douglas Macgregor (@DougAMacgregor) March 18, 2026
Global Analysis Reveals Up to 4 in 10 Cancer Cases Could Be Prevented
Cancer is often talked about as though it strikes at random — a matter of bad luck or inherited genes. But a sweeping new global analysis suggests otherwise. Published in Nature Medicine, the study from the World Health Organization and its International Agency for Research on Cancer (IARC) examined how much of the world’s cancer burden traces back to causes that are, in principle, avoidable.1
The findings reframe cancer less as an inevitability and more as a condition shaped by everyday exposures — what you breathe, drink, eat, and absorb over decades. The researchers’ conclusions carry enormous practical weight, because if a risk factor can be identified and measured, it can also be reduced. What follows is a breakdown of exactly how the analysis reached its conclusions, which exposures drive the most harm and what you can do to act on the data.
Global Data Show Where Cancer Risk Starts
For the study, researchers used data covering 36 cancer types across 185 countries and evaluated 30 risk factors that people and governments can address. They applied a statistical method that estimates how many cases would not occur if a risk factor were removed to determine how much of the global cancer burden traces back to specific exposures. This was not a small regional snapshot. It was a global audit of preventable cancer.
• More than one-third of new cancers were tied to modifiable causes — The investigators found that 7.1 million of 18.7 million new cancer cases in 2022 — 37.8% — were attributable to preventable risk factors. Among men, 45.4% of new cases were linked to these exposures, compared to 29.7% in women. That gap alone tells you something powerful: exposure patterns matter.
If nearly half of cancers in men connect to modifiable behaviors or environments, then your daily exposures shape long-term outcomes.
• Smoking dominated the preventable cancer landscape — Tobacco smoking accounted for 15.1% of all new cancer cases globally, making it the single largest contributor identified in the study. In men, smoking was responsible for an estimated 23% of new cancer cases, while in women it accounted for 6%.
This means smoking’s effect in men was nearly four times higher than in women. The numbers reflect cumulative DNA damage caused by carcinogens in tobacco smoke that trigger mutations and drive tumor formation. If smoking were removed, roughly 15% of global cancer cases would not occur.
• Infections and alcohol formed the next major tier of risk — Infections contributed 10.2% of global cancer cases, and alcohol consumption accounted for 3.2%. Among women, infections were responsible for 11% of new cancer cases — higher than smoking in that group.
That figure underscores how viruses and bacteria such as human papilloma virus (HPV) and Helicobacter pylori (H. pylori) reshape cancer risk through chronic inflammation and long-term cellular damage. Alcohol, by contrast, increases exposure to acetaldehyde, a toxic breakdown product that injures DNA and interferes with repair systems.
• Three cancer types made up nearly half of preventable cases — Lung, stomach and cervical cancers represented nearly 50% of preventable cancer cases globally. Lung cancer was linked primarily to smoking and air pollution. Stomach cancer largely traced back to H. pylori infection.
Cervical cancer was linked to HPV, but it’s important to note that, in most cases, only long-term, untreated HPV infections will trigger cervical cancer, and these are typically easily caught and treated with regular Pap smears.
• Regional differences exposed how environment shapes risk — Preventable cancers ranged from 24.6% to 38.2% in women depending on region and from 28.1% to 57.2% in men. East Asia showed the highest preventable cancer burden among men at 57%, while Latin America and the Caribbean showed the lowest at 28%.2
These differences reflect varying exposure to tobacco, infections, occupational hazards, and environmental pollutants. Where you live influences what you inhale, consume and encounter. The researchers concluded that “strengthening efforts to reduce modifiable exposures remains central to global cancer prevention.”
How to Reduce Your Preventable Cancer Risk
The data show that cancer risk is closely associated with what you inhale, drink, absorb, and store in your tissues. That means your strategy need to begin at the source. Focus first on removing metabolic stressors that damage mitochondria and drive inflammation, because cellular energy failure creates the environment where disease spreads. When you correct that terrain, you shift your long-term trajectory in a measurable way. Here are five steps you can take.
1. Shift your macronutrient balance toward carbs and away from excess fat — If your fat intake approaches 60% of daily calories, you force your body to rely heavily on fat for fuel. That metabolic state drives dysfunction and fuels disease spread, including cancer.3 Keep your fat intake between 30% and 40% of daily calories and aim for about 250 grams of healthy carbohydrates daily.
Build your meals around whole fruit, cooked root vegetables, white rice, healthy protein, and small amounts of well-tolerated whole grains if your gut handles them well. If your digestion struggles, begin with easier-to-digest carbohydrates like fruit and white rice and progress slowly. Your goal is steady glucose use, strong mitochondrial function and lower inflammatory signaling — chemical alarm signals that, when chronically elevated, create conditions favorable to tumor growth.
2. Eliminate vegetable oils and drive linoleic acid (LA) under 5 grams per day — The problem is not just fat. It’s LA, a polyunsaturated fat found in seed oils. High LA intake disrupts mitochondrial energy production, weakens your immune system’s ability to detect and destroy abnormal cells, and activates clotting factors that help tumors establish blood supply and spread.
Remove canola, corn, soybean, safflower, sunflower, and grapeseed oils from your kitchen. Replace them with grass fed butter, ghee or tallow.
For example, instead of sautéing vegetables in canola oil, cook them with ghee. Instead of store-bought salad dressing, use lemon juice and grass fed butter. Use olive oil and avocado oil sparingly, if at all, because they often contain hidden seed oils and high monounsaturated fat that stresses mitochondria.
You’re probably eating more LA than you think. When my Mercola Health Coach app launches, the Seed Oil Sleuth feature will help you track this down to the tenth of a gram. Aim for under 5 grams of LA daily, ideally under 2 grams.
3. Reduce inflammatory drivers by improving body composition and movement — Excess body fat releases inflammatory chemicals that support tumor growth. If you carry weight around your midsection, focus on restoring carbohydrate balance rather than crash dieting. Eat enough protein — about 0.8 grams per pound of ideal body weight, or 1.76 grams per kilogram — with one-third from collagen sources like bone broth.
This protects muscle mass while improving metabolic flexibility, your body’s ability to switch smoothly between burning glucose and fat for fuel. Commit to daily walking and avoid overdoing intense exercise. A sedentary body is a metabolically stagnant one — without regular movement, insulin sensitivity drops, inflammatory markers rise, and mitochondria lose their capacity to burn fuel efficiently.
At the same time, excessive high-intensity training spikes stress hormones and strains recovery. Working your way up to a one-hour brisk walk outdoors daily supports mitochondrial function, improves insulin sensitivity and reduces systemic inflammation.
If you’re starting from minimal activity, begin with 15 to 20 minutes a day and add five minutes per week. Add strength training two or three times per week, but don’t overdo intense sessions. If you feel wired, depleted or unable to recover, you’re pushing too hard. Daily movement builds resilience. Chronic overexertion breaks it down.
Making sure your vitamin D levels are optimized is also important. Multiple large-scale analyses link sufficient vitamin D to lower risk of colorectal, breast and other cancers.4
The mechanisms align with everything discussed in this article — vitamin D modulates immune function, supports your body’s ability to trigger programmed death in abnormal cells and helps regulate the inflammatory signaling that drives tumor growth. Test your blood levels twice a year and aim for 60 to 80 ng/mL (150 to 200 nmol/L).
Many people need supplemental vitamin D3, particularly during winter months or if they spend limited time outdoors. If you supplement, take it with a fat-containing meal to improve absorption, and pair it with magnesium and vitamin K2 to support proper calcium metabolism.
4. Lower chronic stress to protect metabolic function — Chronically high cortisol — your body’s main stress hormone — drives stubborn belly fat, suppresses immune function, and impairs the mitochondrial repair processes your body relies on to prevent abnormal cell growth. Lowering cortisol isn’t a luxury. It’s a metabolic intervention.
Start with slow, deep breathing several times a day and get early morning sunlight to reset your cortisol rhythm. Include healthy carbohydrates with your meals to stabilize energy and calm your nervous system.
Simple pleasures matter, too — laughter, music, time with pets, and doing something you genuinely enjoy all trigger measurable biochemical shifts that lower cortisol and signal safety to your brain. For deeper support, natural progesterone is one of the safest and most effective ways to block cortisol’s harmful effects, helping your body recover from stress overload and reestablish hormonal balance.
In addition, sleep is one of the most overlooked cancer-prevention tools. IARC classifies disrupted circadian rhythms as a probable carcinogen, and the reasons connect directly to the mechanisms discussed throughout this article — sleep deprivation impairs your body’s ability to repair damaged DNA, suppresses natural killer cells that hunt down abnormal cells and elevates the very cortisol you’re working to lower.
Prioritize seven to nine hours of uninterrupted sleep in a dark, cool room. Avoid screens for at least an hour before bed, dim lights after sunset, and keep a consistent sleep and wake time — even on weekends — to anchor your circadian rhythm.
5. Eliminate alcohol and smoking completely and remove other modifiable exposures — Alcohol acts as a metabolic poison and increases cancer burden, much like LA. When you drink, your liver converts ethanol into acetaldehyde, a toxic aldehyde that damages cell membranes and DNA. LA follows an almost identical route. As LA breaks down, it forms another toxic aldehyde called 4-hydroxynonenal (4-HNE).
Both acetaldehyde and 4-HNE are highly reactive molecules that attach themselves to proteins, phospholipids, and mitochondrial DNA, disrupting your body’s ability to generate adenosine triphosphate (ATP) — the energy currency that powers every function in your body, from heartbeat to DNA repair. Think of acetaldehyde and 4-HNE as molecular rust.
They corrode the very machinery your cells use to produce energy, leaving mitochondria damaged and inefficient. So, if you drink, stop. If you smoke, also stop. Address chronic infections where possible and limit exposure to environmental toxins like air pollution as much as possible. If you live near a busy road or in an area with poor air quality, run a HEPA air purifier in the rooms where you spend the most time, especially your bedroom.
When you walk or exercise outdoors, choose routes away from heavy traffic. Filter your drinking water with a high-quality system that removes chlorine, heavy metals, and industrial contaminants. Switch household cleaning and personal care products to versions free of synthetic fragrances, parabens, and phthalates. You don’t need to overhaul everything overnight — start with the exposures you encounter most frequently and work outward from there.
FAQs About Preventable Cancer Risk
Q: How much of cancer is actually preventable?
A: A large global analysis published in Nature Medicine found that roughly four in 10 new cancer cases worldwide are linked to modifiable risk factors.5 That means a significant share of the global cancer burden is tied to exposures such as smoking, alcohol, infections, excess body fat, and environmental pollutants rather than fate or genetics alone.
Q: What are the biggest preventable drivers of cancer?
A: Tobacco smoking ranks as the leading contributor worldwide. Infections such as HPV and H. pylori follow closely behind. Alcohol consumption also adds measurable risk. Lung, stomach, and cervical cancers account for nearly half of preventable cases globally, largely driven by these exposures.
Q: Why does body fat and metabolic health matter for cancer risk?
A: Excess body fat releases inflammatory chemicals that create a biological environment that supports tumor growth. Metabolic dysfunction also impairs mitochondrial function — your cells’ ability to produce energy efficiently. When your mitochondria can’t produce energy efficiently, your cells shift into a stressed, inflammatory state — and that’s precisely the environment where cancer cells thrive.
Q: How does diet influence cancer risk at the cellular level?
A: High intake of seed oils rich in LA and excess fat intake disrupt mitochondrial function and increase formation of toxic aldehydes that damage proteins, membranes and mitochondrial DNA. In contrast, balancing fat intake, prioritizing digestible carbohydrates and eliminating seed oils reduces metabolic stress and lowers inflammatory signaling.
Q: What practical steps reduce preventable cancer risk?
A: Stop smoking and eliminate alcohol. Remove seed oils to lower total LA intake. Maintain a balanced macronutrient profile with adequate carbohydrates and protein. Improve body composition through daily walking and moderate strength training rather than extreme dieting or overtraining. Address chronic infections and reduce exposure to environmental toxins whenever possible.
Test Your Knowledge with Today’s Quiz!
Take today’s quiz to see how much you’ve learned from yesterday’s Mercola.com article.
Which gut cell type ramps up serotonin output during a high-fat diet?
Enterochromaffin cells
Enterochromaffin cells generate most of the body’s serotonin, and high-fat diets push them into overproduction while reducing the serotonin transporter’s clearing capacity. Learn more.
Goblet cells
Paneth cells
Stem cells
Are Sound Machines Bad for Sleep? This New Research Might Surprise You
Most people turn on a sound machine at bedtime because to them it brings comfort. The sound feels like an easy fix for restless nights, and the instant sense of calm makes it even more tempting to depend on night after night. But does that comforting hum actually improve your sleep — or is it secretly working against the brain repair you’re trying to achieve?
A recent study offers a wake-up call: Apparently, sound machines may lead to a noticeable drop in rapid eye movement (REM) sleep. To put it simply, the nighttime sound that seems soothing might actually be pressuring your brain to work through constant auditory input instead of repairing itself.
These findings challenge the assumption that any calming sound is automatically helpful and set the stage for a deeper look at how sound machines might be working against the very sleep quality you’re trying to protect. Before we go into the findings of the study, let’s briefly discuss how sound machines work.
A Primer on Sound Machines
Sound machines are devices designed to produce a steady stream of background noise that help “fill in” the silence of a room. Many people use them as part of a nighttime routine, especially in environments where sudden or unpredictable sounds may interfere with rest. Rather than relying on a phone app — which can introduce disruptive blue light — sound machines offer a dedicated way to create soothing audio throughout the night.
• Why does a sound machine affect your sleep quality? The answer lies in how the brain processes noise. The fact is that even when you’re at rest during deep sleep, your brain still continues to register noise all around you. Unexpected sounds such as traffic, snoring, pets moving around, or household creaks can trigger brief awakenings or shifts between sleep stages, even if you don’t fully remember waking up.
• A sound machine helps reduce the impact of these disruptions — It provides a stable auditory backdrop. The steady hum it emits smooths out the chaos of a noisy house, an anxious mind, or the unpredictable sounds of cars passing by on the street.
• Sound machines may include a variety of sound options — Some play nature sounds, like rainfall, thunderstorms, beach waves, or frogs at night. Others play white noise, which resembles static and contains all audible frequencies at equal intensity. There’s also what’s called pink noise, which is a softer, deeper static sound that resembles steady rushing water. White and pink noise, along with other types like brown and blue, are also referred to as broadband noise.1
Most research suggests that sound machines are generally safe. Even the National Sleep Foundation (NSF) recognizes that sound machines or “sound conditioners,”2 can help both adults and newborns sleep more soundly. However, if used improperly, pink noise machines may not be completely harmless.
What Does the Newest Research Actually Say About Pink Noise and Sleep?
A more recent report published in the journal Sleep provides more insight into how sound machines may be unknowingly harming your nighttime slumber. Conducted by researchers from the University of Pennsylvania Perelman School of Medicine, the study looked at how different noise conditions, including pink noise, shaped the way the brain moved through deep sleep and REM sleep during the night.3 According to an article from Science Daily:
“During a typical night, the brain cycles repeatedly through deep sleep and REM sleep. Deep sleep plays a key role in physical recovery, memory processing, and the removal of waste products from the brain. REM sleep, often referred to as dream sleep, supports emotional regulation, motor skill development, and brain growth.”4
The researchers’ goal was to understand whether the sounds many people rely on each night improve sleep architecture (the natural structure and cycling of your sleep stages) or disrupt it in ways most users never notice.
• The study followed 25 healthy adults, ages 21 to 41, in a controlled sleep laboratory — Most of them were women, and none had any sleep disorders or had previously used sound machines. For seven consecutive nights, they slept for eight hours, from 11 p.m. to 7 a.m.
• The participants were exposed to different conditions — As they slept, they were placed under varying noise conditions, such as environment noise (sounds of aircraft, cars, baby crying, and alarms), pink noise alone, a combination of environment and pink noise, and environment noise while wearing earplugs.
There were also participants who were allowed to sleep in a quiet environment without any noise exposure (the control group). The researchers used overnight polysomnography, which is considered the gold standard for sleep measurement, to capture the data. This is a comprehensive overnight test that measures brain waves, oxygen levels, heart rate, and eye movements.
• As expected, environmental noise significantly reduced deep sleep and increased nighttime awakenings — The participants exposed to this type of noise lost an average 23 minutes of “N3” deep sleep (considered the deepest and most restorative sleep stage) per night. Even if they didn’t remember waking up in the middle of their slumber, their brain activity reflected shallower, more disrupted sleep. They also felt more tired, stressed, and mentally drained the next morning.
• But what was surprising was the effect of pink noise on deep sleep — Pink noise alone, which was played at 50 dB (imagine the sound of moderate rainfall), caused a significant reduction in REM sleep — nearly 19 minutes of sleep lost per night. Over a week, that’s more than two hours of REM sleep lost.
According to the researchers’ findings, this type of noise interferes with the brain circuits that normally allow REM sleep to begin and continue, so instead of creating a restful background for sleep, it may act as a continuous stimulus that alters the brain’s ability to cycle naturally into REM. Your brain doesn’t fully “turn off” during sleep — it still monitors your environment. Pink noise may keep the auditory processing centers partially active, preventing the full transition into REM.
• Why disrupted REM sleep has a significant effect on your health — Chronic REM deprivation doesn’t just make you tired; it also impairs emotional regulation, weakens memory consolidation, and may even accelerate cognitive decline over time. Mathias Basner, M.D., Ph.D., professor of Sleep and Chronobiology in Psychiatry and the study lead author, explained:
“REM sleep is important for memory consolidation, emotional regulation, and brain development, so our findings suggest that playing pink noise and other types of broadband noise during sleep could be harmful — especially for children whose brains are still developing and who spend much more time in REM sleep than adults.”5
What’s even more damaging was when pink noise was combined with environment noise — When paired together, the effects became more pronounced. Both deep and REM sleep were significantly reduced, and participants spent about 15 additional minutes awake during the night. Notably, this increase in wakefulness did not occur with aircraft noise alone or pink noise alone.
So, Should You Ditch Your Sound Machine?
These study findings are vital, as many people today use broadband noise not just for sleep, but also as a relaxation tool throughout the day. Case in point: White noise and ambient podcasts now total about 3 million listening hours per day on Spotify. Meanwhile, the top five “white noise” videos on YouTube have collectively been viewed more than 700 million times.6 Even so, research on how broadband noise affects sleep remains limited and inconclusive.
• Consistent REM disruptions are more damaging than you think — People whose REM sleep is always disrupted have a higher risk of developing mental health issues like depression and anxiety and even Parkinson’s disease. What’s more, majority of people today, particularly adults, are sleep deprived. This means that every minute of REM sleep matters.
• Use sound machine as a tool, not a mandate — If sound machines work for you, then use them in a smart and strategic manner. Basner recommends playing it at a low volume and setting a timer instead of letting it play through the night. “I don’t want to discount that there may be something behind it, because so many people are using it,” he added.7
• Wearing earplugs is a better way to improve sleep quality — This is a simpler — and more cost-friendly — strategy to shut off disruptive noise at night. Around 16% of Americans wear earplugs during bedtime to get the restful sleep they need.8
In the featured study, earplugs restored about 72% of the deep sleep that environmental noise had taken away. That’s equivalent to nearly 17 minutes of N3 deep sleep restored. In nearly every measurement, including sleep stages, awakenings, sleep depth, and morning mood, sleeping with earplugs looked far more similar to sleep during the quiet control night than to any noise-exposed condition.
• Earplugs performed well even during repeated noise events throughout the night — Only at the loudest level tested, 65 dB (which is similar to a noisy vacuum cleaner or busy street heard from indoors), did the protective effect begin to weaken.
• Participants also found earplugs comfortable — Even though the researchers used ordinary foam earplugs for this test, the participants still reported that they slept better with them. This is notable, since comfort and usability often limit whether people stick with sleep tools long-term.
“It is likely that both comfort and sound attenuation could be further improved by using high-fidelity or even custom-fit earplugs instead, although this would have to be shown,” the researchers added.9
Are Sound Machines Safe for Babies and Kids?
During the first weeks of life, newborns spend the majority of their time sleeping — In fact, newborns are recommended to get around 14 to 17 hours of sleep per day, according to the National Sleep Foundation (NSF). This means that these young children spend significantly more time in REM sleep than adults.
• Many parents place sound machines beside their newborns’ or toddlers’ beds — They do this with the best of intentions, to help their children fall asleep and stay asleep through the night. However, based on the featured research, this habit could be doing more damage, as they are more susceptible to the possible harms of pink noise exposure.
• REM sleep loss may be more pronounced in young children — Although the study did not observe the effects of broadband noise on these age groups, the researchers still warn parents to be careful in using sound machines until there’s more conclusive research on their effects on younger brains.
“Overall, our results caution against the use of broadband noise, especially for newborns and toddlers, and indicate that we need more research in vulnerable populations, on long-term use, on the different colors of broadband noise, and on safe broadband noise levels in relation to sleep,” Basner said.10
• The volume level of the machine is also a concern — Excessively high volumes can pose risks over time. One study published in the National Library of Medicine reported that white noise played above recommended limits may negatively affect young children’s hearing and language development.11
For context, the safe noise level for hospital nurseries is around 50 decibels (dB). For adults, white noise is typically regarded as safe between 50 and 70 dB. Beyond that range, hearing protection may be necessary to reduce the risk of long-term damage.12
To summarize, below is a comparison of the different types of broadband noises made by sound machines and the recommendations based on the research findings.
Noise type
Sound profile
Effect on sleep
Recommendation
Pink noise
Softer, deeper static (like steady rainfall or rushing water)
Reduced REM sleep by ~19 minutes per night in lab settings
Use cautiously, especially for children whose brains need more REM sleep
White noise
Even static across all frequencies (like TV static or a fan)
Masks disruptive sounds but shows no clear benefit for sleep quality
Keep volume low (50 to 70 dB), use a timer, place device 3+ feet away
Brown noise
Deep, rumbling static (like thunder or strong wind)
Limited research available; effects on sleep architecture unclear
Apply same safety precautions as pink/white noise until more data exists
How to Use a Sound Machine Safely
If you’re not ready to give up your sound machine entirely, you can still minimize the risks. Here’s a practical, research-aligned setup guide you can implement tonight:
1. Use the lowest effective volume — Set your sound machine to the minimum level that still masks your specific trigger noises, like traffic or snoring. Lower loudness means less risk of disrupted sleep over time. Aim for 50 dB or below — roughly the volume of light rainfall.
2. Increase the distance from your bed — Place the device across the room, not on your nightstand. Sound pressure decreases with distance, so moving your machine even 3 to 6 feet farther from your ears significantly reduces exposure while still providing masking benefits.
3. Set a sleep timer or auto-off feature — You don’t need broadband noise running all night. Set a timer for 30 to 60 minutes — enough time to fall asleep. Once you’re in deep sleep, your brain is less sensitive to moderate environmental sounds anyway.
4. Consider earplugs as an alternative — In the featured study, simple foam earplugs restored about 72% of the deep sleep lost to environmental noise, outperforming pink noise in nearly every measurement. Try them instead of, or alongside, your sound machine.
5. Combine with physical noise control — Address noise at the source: heavy curtains, door sweeps, draft stoppers, and soft furnishings all reduce sound transmission. These passive solutions don’t carry the REM-disruption risks of continuous broadband noise.
6. Run a one-week self-experiment — If you wake up groggy despite “sleeping” seven to eight hours, try removing your sound machine for one week. Track your morning alertness, mood, and energy. If you feel more restored without it, that’s your answer.
Frequently Asked Questions (FAQs) About Sound Machines and Sleep
Q: Can pink noise disrupt rapid eye movement (REM) sleep?
A: Yes, recent controlled sleep-lab research suggests pink noise may reduce REM sleep, which is the stage associated with dreaming, memory consolidation, emotional regulation, and brain development. In laboratory conditions, participants exposed to pink noise experienced a measurable reduction in REM sleep compared to quiet conditions.
While pink noise is often marketed as calming, continuous broadband sound may act as an ongoing auditory stimulus that subtly interferes with the brain’s natural sleep cycling. The effect may be especially relevant for people already struggling with sleep quality or those who rely on noise all night at moderate volumes.
Q: What is a safe decibel level for sleep?
A: For most adults, sleep experts generally recommend keeping nighttime sound exposure around 50 decibels (dB) or lower — roughly the sound of light rainfall. Some guidance considers 50 to 70 dB acceptable for adults, but lower is better when possible. For infants and young children, caution is even more important, and volume should remain at or below nursery safety standards (around 50 dB).
Q: Are sound machines safe for babies?
A: Parents should use caution. Babies spend significantly more time in REM sleep than adults, and REM plays a critical role in brain development. Emerging research suggesting that certain types of broadband noise may reduce REM sleep raises questions about prolonged overnight use in infants and toddlers. Additionally, excessive volume may pose hearing risks over time.
Environmental fixes — such as blackout curtains, soft furnishings and white-noise alternatives at low levels — may be safer first-line options.
Q: Where should I place a sound machine in the bedroom?
A: Placement significantly affects sound exposure. For safer use, position the device across the room, not on your nightstand. Keep it at least 3 to 6 feet away from your bed or your child’s crib. Use the lowest volume that masks your triggers, and never direct the speaker toward your ears. Sound intensity drops as distance increases, so moving the machine farther away reduces the decibel level reaching your ears while still providing masking benefits.
Q: Do I need a timer or should a sound machine run all night?
A: For many people, running a sound machine all night is unnecessary. Once you fall asleep — especially after entering deeper sleep stages — your brain becomes less sensitive to moderate background sounds. Using a 30- to 60-minute timer may reduce potential REM disruption and limit prolonged noise exposure. Continuous overnight use may not provide added benefit and could increase the risk of sleep-stage interference.
Q: What’s the difference between pink, white and brown noise?
A: The “color” of noise refers to how sound frequencies are distributed:
• White noise — Equal intensity across all audible frequencies; sounds like steady static or a fan.
• Pink noise — Emphasizes lower frequencies; softer and deeper, often compared to rainfall or rushing water.
• Brown noise — Even more weighted toward low frequencies; deeper, rumbling sound similar to thunder.
Pink noise has recently drawn attention due to findings suggesting it may reduce REM sleep in certain lab settings. White and brown noise are widely used for sound masking, but high-quality evidence comparing long-term effects on sleep architecture remains limited.
Q: Are there alternatives to sound machines that are safer?
A: Yes. Depending on the source of nighttime noise, alternatives may better preserve sleep quality:
• Earplugs — In laboratory studies, earplugs protected deep sleep more effectively than pink noise during aircraft noise exposure.
• Physical soundproofing — Door sweeps, draft stoppers, heavy curtains and rugs can reduce environmental noise without continuous auditory stimulation.
• Fans or air purifiers at a distance — Provide gentle masking without placing a speaker near your head.
• Behavioral sleep strategies — Consistent bedtime, light control and stress reduction may reduce the perceived need for artificial noise.
If you wake feeling groggy despite adequate sleep duration, consider a one-week trial without broadband noise to assess how your body responds.
The Surprising Role of Cortisol in Alzheimer’s
A New Series of Health Insights Is on the Way
WAŻNY
A New Series of Health Insights Is on the Way
Our team has been working behind the scenes to prepare new research and practical health
strategies for our readers. While we finish preparing what’s coming next, we invite you to
explore one of the most-read articles from our library below. See exactly what’s changing →
Alzheimer’s disease doesn’t begin with memory loss — it begins years earlier with a slow, silent shift in your body’s stress chemistry. Long before neurons die, your brain’s hormonal balance starts to erode under constant pressure from everyday stress. The same hormones that once kept you alert and focused start working against you, wearing down your brain’s repair systems and disrupting the flow of energy your cells depend on.
Cortisol, the body’s main stress hormone, plays a central role in this process. When it stays high for too long, it drains your metabolic reserves and interferes with memory formation. Meanwhile, a second hormone called DHEA-S acts as cortisol’s natural counterbalance, helping protect neurons and stabilize brain function.
When the ratio between these two hormones tilts toward cortisol, your brain loses its resilience and becomes more vulnerable to aging and degeneration. This hormonal tug-of-war — shaped by stress, diet, and metabolism — has drawn new attention from researchers exploring why some people develop Alzheimer’s while others do not. The latest findings suggest that long-term hormonal imbalance, not just genetics or plaque buildup, could be one of the earliest warning signs of decline.
Understanding this relationship changes how you think about prevention. By strengthening your metabolism, restoring hormonal balance, and reducing chronic stress, you can support your brain’s ability to heal and adapt — long before symptoms appear. The new research provides a roadmap for how to start.
Stress Hormones Tip the Balance Toward Alzheimer’s
A clinical study published in Cureus examined 85 adults in Serbia — 45 with diagnosed Alzheimer’s disease and 40 healthy peers of similar age and sex — to determine how two hormones, cortisol and DHEA-S, relate to brain health.1 Cortisol is your body’s main stress hormone, while DHEA-S (dehydroepiandrosterone sulfate) acts as its built-in counterbalance — a neurosteroid that supports brain resilience and energy metabolism.
Unlike DHEA, which is the fast-acting, active form, DHEA-S is its sulfated storage form that circulates in your blood far longer and provides a more stable picture of long-term stress balance. By focusing on DHEA-S, the researchers could better gauge chronic stress effects on the brain rather than short-term fluctuations. The scientists wanted to know whether Alzheimer’s patients showed measurable differences in these hormones or in their ratio, which indicates how well your body manages prolonged stress.
• People with Alzheimer’s had higher cortisol levels but not lower DHEA-S — Those with Alzheimer’s showed cortisol levels averaging nearly 399 nanomoles per liter (nmol/L) — about 20% higher than healthy adults — yet their DHEA-S concentrations stayed roughly the same.
This imbalance means the stress response remains chronically activated without the brain’s natural protection. When cortisol dominates, neurons experience more inflammation and less regeneration. The study also noted that this skewed balance was strongest among participants aged 65 to 75, suggesting that middle-to-late adulthood is when stress hormones begin exerting their most damaging effects.
• The cortisol-to-DHEA-S ratio proved to be the real warning sign — Although each hormone alone tells part of the story, the researchers emphasized that their ratio — how much cortisol outweighs DHEA-S — offers a clearer window into chronic stress and brain decline.
In Alzheimer’s patients, that ratio climbed steeply, implying that the body’s defense system against cortisol’s toxicity was failing. This finding helps explain why some people with normal cortisol readings still experience cognitive decline: it’s the imbalance, not just the level, that matters.
• Men and women responded differently, revealing hormonal sensitivity — In healthy adults, men had significantly higher DHEA-S levels than women, meaning their brains could have greater protection from chronic stress. But that sex difference disappeared in those with Alzheimer’s.
The disease seemed to override normal hormonal patterns, flattening DHEA-S levels in both sexes. This means that once neurodegeneration begins, your brain’s ability to maintain hormonal balance — one of its self-defense tools — breaks down.
• Age changed the picture again, suggesting a nonlinear hormonal response — When researchers divided participants by age, they noticed that younger Alzheimer’s patients (60 to 65) had higher DHEA-S levels, which dropped sharply in the 66 to 75 group before rising again after age 75.
This unexpected curve points to a possible window of hormonal collapse, where midlife stress overwhelms the body’s compensatory systems. If you’re in this age range and facing chronic stress, that’s when intervention — stress reduction, adequate rest, and metabolic support — could be most protective for your brain.
Cortisol Acts Like an Overzealous Cleanup Crew That Damages What It’s Meant to Protect
Elevated cortisol increases inflammation and oxidative stress — chemical reactions that corrode neurons and disrupt communication between brain cells. It also suppresses the growth of new neurons in your hippocampus, the brain’s memory center, making it harder to store new information.
In contrast, DHEA-S supports neuronal survival, enhances energy metabolism, and shields brain tissue from the harmful effects of excessive cortisol. When cortisol wins this hormonal tug-of-war, brain networks lose their flexibility and begin to deteriorate.
• Why stress and memory loss are so tightly linked — Chronic cortisol elevation interferes with glucose uptake in brain cells, depriving them of the fuel needed to form memories. It also increases amyloid-beta and tau accumulation — the same proteins that define Alzheimer’s pathology.
Meanwhile, DHEA-S helps counter these effects by enhancing insulin sensitivity and calming overactive immune responses in your brain. In simple terms, one hormone burns your mental circuits, the other repairs them.
• A new biological marker for early intervention — Instead of waiting for memory loss or imaging changes, tracking your cortisol-to-DHEA-S ratio could signal early stress damage years before cognitive symptoms arise.
If your cortisol stays high while DHEA-S falls or stagnates, that’s a red flag. Supporting your metabolic health, prioritizing quality sleep, and restoring hormonal balance could help keep your brain’s internal environment stable long before Alzheimer’s develops.
Lowering Cortisol and Raising Metabolic Energy Could Reverse Brain Decline
In a commentary, bioenergetic researcher Georgi Dinkov analyzed the Cureus study showing that people with Alzheimer’s disease had significantly higher cortisol levels and a skewed cortisol-to-DHEA-S ratio compared to healthy adults.2 He explained that these results validate decades of bioenergetic research linking chronic stress, low metabolism, and neurodegeneration.
Dinkov emphasized that it’s not just elevated cortisol that drives decline — it’s the imbalance between cortisol and protective steroids such as DHEA, testosterone, and progesterone. When this ratio tips toward cortisol dominance, your body remains in a chronic “fight-or-flight” state that accelerates tissue breakdown and cognitive loss.
• Dinkov connected the findings to thyroid-driven metabolic stress — Building on the Cureus data, Dinkov explained that hypothyroidism — a sluggish thyroid that slows metabolic energy production — creates the same hormonal pattern seen in Alzheimer’s patients: high cortisol and suppressed DHEA-S.
When your metabolism slows, your body compensates by ramping up stress hormones to stay alert and energized. But this backfires over time, leading to chronic brain inflammation, poor glucose uptake, and reduced adenosine triphosphate (ATP) production — the energy currency your brain depends on.
• Your cortisol-to-DHEA-S ratio predicts long-term health better than any single hormone — According to Dinkov, this ratio — spotlighted by the Cureus research — is among the strongest predictors of all-cause mortality and neurodegenerative risk. Even when cortisol fluctuates throughout the day, the ratio reveals whether your stress and repair systems are balanced.
Dinkov suggested measuring cortisol and DHEA-S in hair or nails rather than blood, since these tissues reflect long-term hormonal patterns. For anyone trying to gauge chronic stress or cognitive risk, this offers a simple, objective biomarker that’s far more reliable than a one-time blood test.
• Natural compounds help restore hormonal balance and metabolic strength — Dinkov referenced several well-known substances — aspirin, niacinamide (vitamin B3), progesterone, pregnenolone, thyroid support, glycine, and emodin — that help correct the same imbalance observed in the Cureus study. These compounds work by lowering excess cortisol, improving mitochondrial energy output, and supporting the production of protective hormones.
Niacinamide, for instance, increases NAD+, which fuels cellular repair, while aspirin dampens inflammation and cortisol overproduction. Used together, these tools shift your body back into a “rest-and-repair” mode rather than the constant stress chemistry that drives brain aging.
• DHEA acts as a built-in cortisol regulator — Dinkov explained one of the key ways DHEA helps keep cortisol in check: it blocks the enzyme that turns inactive cortisol back “on” and boosts the one that clears excess cortisol from your body. This dual action makes DHEA a natural cortisol buffer that prevents the overactivation of stress pathways.
In other words, DHEA gives your brain a biochemical “cooling system,” stopping cortisol from overheating your neurons. Supporting DHEA through thyroid health, nutrition, and targeted supplementation helps restore this essential balance.
• Stress is a symptom of low energy, not just emotional strain — Dinkov described how the elevated cortisol levels observed in the Cureus Alzheimer’s cohort represent a deeper issue: energy failure. When your cells don’t make enough ATP — whether from poor thyroid output, nutrient deficiencies, or aging — they turn to cortisol to compensate.
The hormone breaks down tissue to release fuel, but that process worsens energy depletion over time. This self-reinforcing loop explains why chronic stress feels endless: it’s a metabolic, not psychological, trap. Dinkov concluded that maintaining a low cortisol-to-DHEA-S ratio protects more than memory — it sustains whole-body resilience.
People who keep this ratio balanced experience better sleep, stable mood, and slower biological aging. His message is practical: by restoring thyroid function, eating enough to prevent energy deficits, and lowering chronic inflammation, you directly influence the biochemical environment that determines whether your brain decays or endures.
Rebuild Your Energy System to Lower Cortisol and Protect Your Brain
If you wake up tired, crash midafternoon, or feel wired when you should be asleep, your body’s stress chemistry has taken over. The Cureus study3 and Dinkov’s review4 both point to the same conclusion: your brain suffers when your cells can’t make enough energy.
To fix that, you have to restore steady fuel, retrain your stress response, and help your body recognize that it’s no longer in survival mode. Here’s how to bring your hormones — and your energy — back into balance:
1. Feed your metabolism the fuel it’s been missing — Cutting carbs keeps your body trapped in a constant stress loop because cortisol spikes whenever blood sugar drops too low. Break that pattern by eating enough healthy carbohydrates — around 250 grams daily — to give your mitochondria a steady energy supply.
Start with gentle foods like fruit and white rice. When your digestion feels stable (no bloating or irregularity), add cooked root vegetables, then more vegetables, legumes, and well-tolerated whole grains. Once your body trusts it’s being fed regularly, cortisol naturally declines, and your energy and focus stabilize.
2. Move in ways that restore instead of deplete — Overdoing endurance exercise or high-intensity intervals keeps your body in fight-or-flight mode long after the workout ends. Cortisol stays elevated, recovery slows, and sleep suffers.
Replace long, punishing sessions with physical activities that build energy rather than drain it — strength training, walking outdoors, dancing, or swimming at an easy pace. Use how you feel afterward as your guide: if you finish feeling grounded and calm, you’ve helped your hormones, not hurt them.
3. Train your nervous system to shift out of stress — Your breath is the fastest lever you have to quiet cortisol and activate your parasympathetic, or “rest and digest,” system. Try rhythmic breathing patterns like 4-7-8 or 4-8 breathing — inhaling for four seconds, holding briefly, and exhaling slowly for seven to eight seconds.
The extended exhale stimulates your vagus nerve, lowering heart rate and cortisol while signaling safety to every organ. Practice before bed, after meals, or whenever tension rises. Over time, your body learns that it no longer needs to live in emergency mode.
4. Rebuild your circadian rhythm through light and sleep — Cortisol follows your light exposure, not your alarm clock. Get outside within an hour of waking to anchor your body’s circadian rhythm, and dim screens and overhead lighting at night so melatonin can rise naturally.
Keep your bedtime and wake-up times consistent — even on weekends — to lock in hormonal balance. Deep, regular sleep clears stress hormones, strengthens memory, and repairs brain tissue. If you’re dragging through the day, fix your light and sleep first instead of relying on caffeine.
5. Use natural progesterone to quiet the cortisol surge — Bioidentical progesterone acts as your body’s built-in cortisol brake, restoring calm where chronic stress has hijacked balance. Unlike synthetic versions, natural progesterone fits perfectly into your body’s own receptor system, lowering cortisol’s overstimulation and supporting deep rest.
FAQs About Cortisol and Alzheimer’s Disease
Q: What did the new Alzheimer’s study reveal about cortisol and DHEA-S?
A: Researchers found that people with Alzheimer’s disease had cortisol levels roughly 20% higher than healthy adults, while their DHEA-S levels stayed about the same. This created a skewed cortisol-to-DHEA-S ratio — meaning stress hormones were overpowering the brain’s natural defenses. That imbalance, not just genetics or amyloid buildup, appears to drive the early stages of brain decline.
Q: How are DHEA and DHEA-S different?
A: DHEA is the fast-acting form of the hormone, while DHEA-S is the stable, long-lasting form stored in your blood. Because DHEA-S changes slowly, it’s a better measure of long-term stress and brain resilience. It also acts as a neurosteroid, helping neurons resist inflammation and oxidative damage while buffering cortisol’s harmful effects.
Q: What did Georgi Dinkov’s analysis add to this research?
A: Dinkov explained that the Cureus study confirms a broader principle: high cortisol and low metabolic energy often go hand in hand. He connected these hormone shifts to thyroid sluggishness, nutrient depletion, and aging — all of which drain cellular energy and raise stress chemistry. He also noted that maintaining a low cortisol-to-DHEA-S ratio predicts not just better memory but longer life and greater overall resilience.
Q: What practical steps help lower cortisol and restore hormonal balance?
A: To calm your stress system, start by fueling your metabolism. Eat enough healthy carbohydrates — about 250 grams per day — to keep blood sugar stable. Cut back on overtraining, use rhythmic breathing to activate your vagus nerve, and rebuild your circadian rhythm by getting morning sunlight and sleeping on a consistent schedule. These changes lower cortisol naturally while improving energy and mental clarity.
Q: How does progesterone fit into this picture?
A: Natural progesterone acts as a built-in cortisol blocker. Your body recognizes it as a calming, balancing hormone that reduces overstimulation, helps you sleep deeply, and stabilizes mood. Natural progesterone effectively blocks cortisol by reducing blood concentrations, helping restore hormonal harmony, protecting your brain and body from the long-term effects of stress.
U.S. Treasury projected to buy back $15 Billion of their own debt today, surpassing last week’s $14.7 Billion purchase as the LARGEST Treasury buyback in history. How can these buybacks continue?
U.S. Treasury projected to buy back $15 Billion of their own debt today, surpassing last week’s $14.7 Billion purchase as the LARGEST Treasury buyback in history. How can these buybacks continue? — Douglas Macgregor (@DougAMacgregor) March 17, 2026
Despite War In Iran, Board Of Peace Moves On In Gaza

The ISF force charged with overseeing security in Gaza seems like strange bedfellows: Morocco, Indonesia, Kosovo, Albania, and Kazakhstan. Four are solidly Muslim, while Kazakhstan is on the fence with a 50% Muslim population. This means that Trump is deepening his relationship with other Islamic nations around the world. If Gaza is an Islamic project, then it will be run by asset-based Islamic (Sharia) finance.
BREAKING: Tanker attacked while anchored in Gulf of Oman.
BREAKING: Tanker attacked while anchored in Gulf of Oman. — Douglas Macgregor (@DougAMacgregor) March 17, 2026
RT by @DougAMacgregor: The US-Israeli war on Iran is the most significant geopolitical event since the fall of the Soviet Union in 1991: the culmination of the rupture in the US-based unipolar order. I spoke w/@proud_diplomat to discuss the war’s system-wide impact. Tune in.
The US-Israeli war on Iran is the most significant geopolitical event since the fall of the Soviet Union in 1991: the culmination of the rupture in the US-based unipolar order. I spoke w/@proud_diplomat to discuss the war’s system-wide impact. Tune in.https://t.co/QrvozTgkW3 — Arta Moeini PhD (@ArtaMoeini) March 16, 2026
RT by @DougAMacgregor: The United States is navigating a fiscal storm that demands a significant course correction in its defense strategy, leadership, and mindset. FULL ARTICLE: ➡️ pic.
The United States is navigating a fiscal storm that demands a significant course correction in its defense strategy, leadership, and mindset. FULL ARTICLE: ➡️https://t.co/THfUGXD0Df pic.twitter.com/wV3MEmYyU6 — Douglas Macgregor (@DougAMacgregor) March 16, 2026
Why Trump’s Takeover In Gaza Preceded The War In Iran

The war in Iran will end. The reconstruction will begin. The financial architecture assembled before the first bomb fell will be deployed at scale — not just in Gaza and Iran, but as the template for every post-conflict territory that follows. The Board of Peace was never just about Gaza. Its charter says its mandate is global. The $1 billion permanent seats are still available.
BREAKING: More than 3,350 Israeli civilian and military personnel have now been injured since start of the Iran war.
BREAKING: More than 3,350 Israeli civilian and military personnel have now been injured since start of the Iran war. — Douglas Macgregor (@DougAMacgregor) March 16, 2026
The Moral Hazards Of War And How They Accelerate Technocracy

Moral hazard is when your brother-in-law borrows your car and drives it like a maniac, because if he wrecks it, it’s your car, not his. The risk is yours. The recklessness is his. And the fact that he faces no downside is exactly what makes him reckless in the first place. Of course, you could be hoping that he totals your car so you can
Happy Birthday, America. Now Hand Over Your Sovereignty.
The 250th anniversary will sport celebrations everywhere as Technocracy and Technocrats slither around to provide the exploding cake. The war with Iran provides emergency powers to do unthinkable and unspeakable things to our nation. Americans are already in a state of shock with the uncertainty of war, which is the perfect scenario for Technocrats to practice the “Science of social engineering.”
Will Yann LeCun Provide The Next Breakthrough In AI?

Mark Zuckerberg just lost his Chief AI Scientist, who is pursuing a $1 billion startup to get AI right. At 65, investors are betting on LeCun. He says that LLMs are at a dead end and increasingly resistant to new breakthroughs. Instead, he says the future of AI rests on meaning, rather than selecting the next word. If an AI can visualize an object or